



In a lab at a MaineHealth office suite in South Portland, Dan Pelletier is part of a team of health care workers across the state doing crucial behind-the-scenes work on a medicine that could help prevent hospitals from being overwhelmed with COVID-19 patients.
Pelletier is a pharmacy technician who prepares monoclonal antibodies for infusion into patients. The antibodies – marketed with the brand name Regeneron – are an increasingly used weapon in the battle against COVID-19 as hospitals around the country experience a deluge of patients caused by the delta surge. There were 204 COVID-19 patients in Maine hospitals on Saturday, one of the highest numbers since the pandemic began.
Demand for the treatment is much bigger than supply. But the antibodies – if they can be more widely used in the coming weeks and months – hold promise to prevent hospitalizations.
“There are very few specific therapies for COVID where the enthusiasm in the medical community has strengthened over time, rather than eroded,” said Dr. Cheryl Liechty, an infectious disease physician and epidemiologist who helped stand up a monoclonal antibody clinic at Pen Bay Medical Center in Rockport. “This is proving to be a useful tool in preventing severe disease.”
Bruce Campbell, director of pharmacy for Central Maine Healthcare in Lewiston, said the antibody treatments are “the most encouraging medication we have to stop the disease’s progression.”
Monocolonal antibodies are laboratory-produced versions of a natural protein and are designed specifically to attack the coronavirus that causes COVID-19.
Pelletier has prepared more of the infusions as the delta variant has swept across the state in recent weeks. Maine clinics and hospitals have been giving the treatment to more patients recently and plan to expand. At the same time, supplies of the medications from the federal government are tightening as demand soars across the country.
Dr. Nirav Shah, director of the Maine Center for Disease Control and Prevention, tweeted on Friday that the nationwide shortage of monoclonal antibodies “will affect Maine. If you were banking on getting monoclonals if you get COVID, they may not be there.”
How long the shortage will last is unclear as the Biden administration moves to ramp up supplies by ordering more doses from manufacturers and by taking over distribution.

Dan Pelletier, a pharmacy technician specialist at Maine Medical Center, demonstrates the process of preparing antibodies used to treat COVID19 patients. Derek Davis/Staff Photographer
Biden administration officials told national news outlets last week, including The Washington Post and CNN, that the concentration of doses in seven states – Florida, Texas, Mississippi, Tennessee, Alabama, Louisiana and Georgia – made up 70 percent of all orders.
“We must work to ensure our supply of these life-saving therapies remains available for all states and territories, not just some,” said an anonymous federal health official quoted in The Washington Post.
The treatment has not been as politicized as vaccines, and southern state governors such as Florida’s Ron DeSantis have promoted antibody treatment while slamming vaccine mandates, including threatening fines for businesses that impose mandates.
Brian Marden, chief pharmacy officer for MaineHealth, said that distribution shifted last week from health care systems ordering directly from suppliers to the Biden administration allocating doses to states. How supplies shape up in the next few weeks could impact planned expansions of monoclonal antibody clinics throughout MaineHealth’s provider network, he said.
“That is certainly a sign of challenges with supply versus demand,” Marden said. “We will have to see how this plays out as demand has certainly gone up drastically across the country, and I don’t have a lens out as to what the supply production outlook is like with manufacturers.”
Supplies have so far largely kept up with demand in some parts of the state, but in northern Maine demand is outstripping supply, according to hospital officials.
USEFUL TREATMENT, BUT NOT A VACCINE REPLACEMENT
The antibodies cost $2,100 per dose but are provided to states for free from the federal government. They help the body mount an immune response and are most effective in patients with mild to moderate disease when given as soon as possible after the onset of symptoms.
There is some discretion by doctors in who gets prescribed monoclonal antibodies, based on rules from the Food and Drug Administration’s emergency use authorization to prescribe the drug. But, in general, it is being used for COVID-19 patients ages 60 and older, or younger people with high-risk conditions, such as obesity, diabetes or conditions that suppress the immune system.
The Maine CDC does not track monoclonal antibody usage. But based on surveys of the major hospital systems in Maine, the outpatient treatment has gone from being used dozens of times per week this spring to hundreds of doses that are now given weekly.
Carol Perry, 74, of Waldoboro got the antibody treatment at Pen Bay in August. Perry’s immune system is suppressed because of chemotherapy treatments she needs for breast cancer and, while she is fully vaccinated, she contracted a breakthrough COVID-19 infection this summer.
“I believe if it wasn’t for that treatment, I would have wound up in the hospital,” said Perry, who was suffering from COVID-19 symptoms of a severe headache, fever, congestion and sinus pain. “I’m just so grateful to have gotten it.”
Perry said she was so weak she needed to use a wheelchair to go to the treatment, but she started feeling better within two days and recovered in a week. She was feeling so well that she was able to visit her grandchildren in Colorado in September.
Public health experts view monoclonal antibodies as a key tool to combat COVID-19, a supplement to vaccines, masking and social distancing. Studies show the antibody treatment can reduce hospitalizations by 50 percent to 70 percent.
Vaccines are 95 percent effective in preventing hospitalizations, and experts say they remain the most important tool in the fight against the virus. They reduce the risk of getting infected and spreading the disease, as well as preventing serious illness. Antibodies are almost always given post-infection, although they could be given to patients at high risk of infection if supplies become a lot more robust.

Amanda Snow, pharmacy manager of Ambulatory Oncology and Infusion Services for MaineHealth Derek Davis/Staff Photographer
“This is not in any way a replacement for the vaccine,” said Amanda Snow, a pharmacy manager for MaineHealth who oversees the monoclonal antibody program for the network, which includes Maine Medical Center in Portland and seven other Maine hospitals. “It’s so important for people to get vaccinated. Hopefully, we are keeping them out of the hospital with monoclonal antibodies, but it’s not a guarantee.”
Vaccines also remain far easier to get. Someone getting a vaccine can be in and out of a clinic within 30 minutes, including a 15-minute waiting period. And there are numerous sites across the state to get a vaccine, including the Auburn Mall mass vaccination clinic, drugstores and doctor’s offices.
Receiving a monoclonal antibody infusion requires three hours and involves delivering the medication into the body intravenously. With fewer places to get an infusion compared with a vaccine, you may need to drive much farther to get into an antibody clinic.
“The best thing you can do to avoid hospitalization is to get vaccinated and prevent getting infected in the first place,” said Dr. James Jarvis, COVID-19 incident commander of Northern Light Health, the parent company of Eastern Maine Medical Center in Bangor and Mercy Hospital in Portland.
Vaccination is increasingly becoming mandatory, with the Biden administration now requiring employers with more than 100 workers to mandate vaccination or have workers get tested weekly. The rule also applies to Maine state and local government workers. In addition, Maine requires health care workers to get vaccinated for COVID-19.
Still, the monoclonal antibodies can be helpful for those who haven’t gotten vaccinated and contract COVID-19, or vaccinated patients with compromised immune systems who contract a breakthrough case. The antibodies have also been shown to be effective as a preventive measure for vulnerable people who come into contact with the disease, but are not in wide use as a prevention tool because of limited supplies.
AVOIDING THE HOSPITAL
Pelletier, dressed in full protective gear, demonstrated how pharmacists are preparing the infusions in sterile labs across the state. Preparing the medication for use takes about five minutes for each dose, and the lab where he works prepares about 40 doses weekly compared with a handful of doses weekly this spring. Throughout the MaineHealth system, antibody treatments fluctuated from about 15-20 per week this spring, to the single digits in the early summer when case counts subsided, to now about 50 per week.
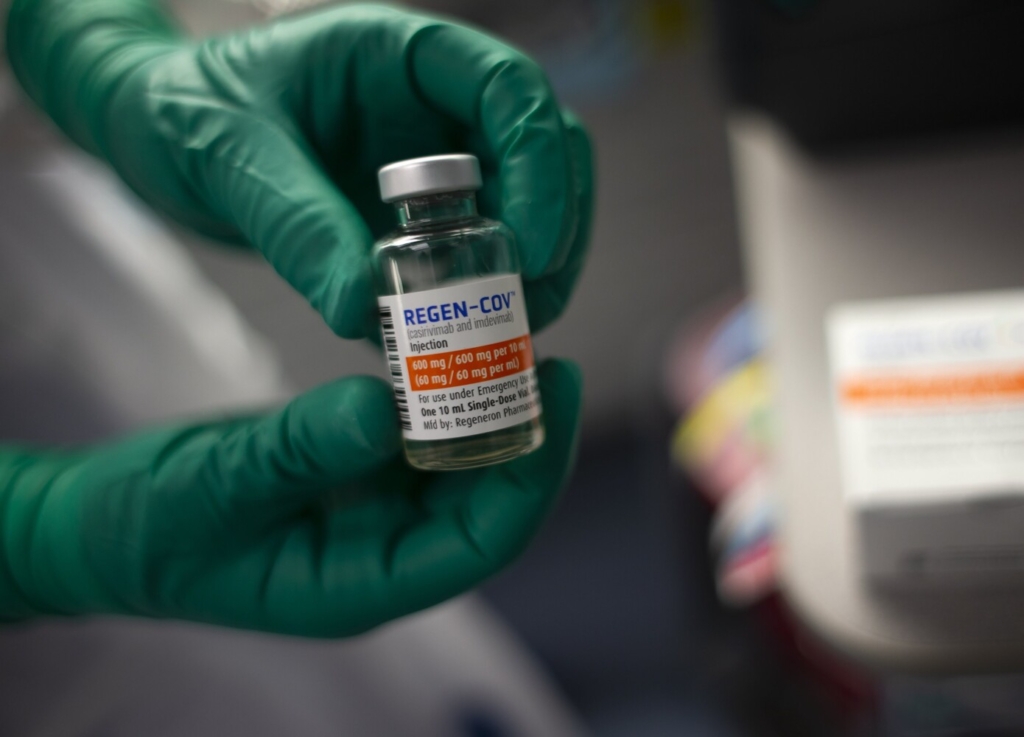
Dan Pelletier, a pharmacy technician for MaineHealth, holds up a vial of monoclonal antibodies. Derek Davis/Staff Photographer
The medication comes in one-dose vials and is stored in a refrigerator at between 2 and 8 degrees Celsius.
Ten milliliters of the medication are injected into an IV bag of sodium chloride. The IV line is connected to a pump that controls the dosing, delivered in a steady drip over 30 minutes to prevent side effects such as nausea, accelerated heart rate and dizziness, said Snow, the MaineHealth pharmacy manager. Counting the time it takes to sterilize rooms, the mandatory one-hour waiting periods and the 30 minutes that the infusion takes, each patient requires about three hours of staff time.
While time-consuming, Snow said, the infusions can prevent hospitalizations and save the many hours, resources and money needed to care for a hospitalized patient. Preventing severe illnesses saves lives and prevents long-term health problems resulting from recovery from hospitalization.
“It’s extremely important to preserve hospital beds,” Jarvis said. “Anything we can do to prevent one more person from needing hospital-level care is one more bed we can use for someone else.”
HOW IT WORKS
Antibodies are proteins produced by the body to fight infections. Monoclonal antibodies are made in laboratories and mimic the body’s immune response, in this case designed specifically to target the COVID-19 virus. Other versions of the treatment have been developed for different viral infections, such as Ebola and rabies, according to the Journal of the American Medical Association.
For COVID-19, the monoclonal antibodies bind to the virus’s spike protein, which can block the virus from invading human cells.
“Instead of depending on the body to develop an immune response, you are supplying the patient with an immune response,” Liechty said.
Vaccines are superior because they cause the immune system to mount a full immune response to the invading coronavirus, including a T cell response that is not produced by monoclonal antibodies, Liechty said.
“T cells also have antibody-like receptors that enable tight binding to specific viral structures, but they are whole cells, some of which – called ‘killer’ T cells – are capable of directly killing virus-infected cells they encounter. T cells therefore have long been regarded as the heavy armor of the immune system,” said an August study by University of Pennsylvania researchers.
Matt Cox, pharmacy clinical coordinator for Central Maine Healthcare, said that monoclonal antibodies – while not as effective as vaccination – can still boost the immune system.
“Essentially we are providing an immune response for them,” Cox said.
Perry, the Waldoboro cancer survivor who received the treatment in August, said she believes the treatments saved her life. Even if she had survived without the treatment, she would have likely had to endure a lengthy and difficult hospitalization, she said. Her husband, Jim Perry, 80, also contracted COVID-19 in a breakthrough case, and the monoclonal antibodies helped him recover as well.
“I might not be here if it weren’t for this treatment,” Perry said.
Send questions/comments to the editors.

Comments are no longer available on this story